Financial impact of quality emergency care: national perspective
Thursday, 17 August 2023
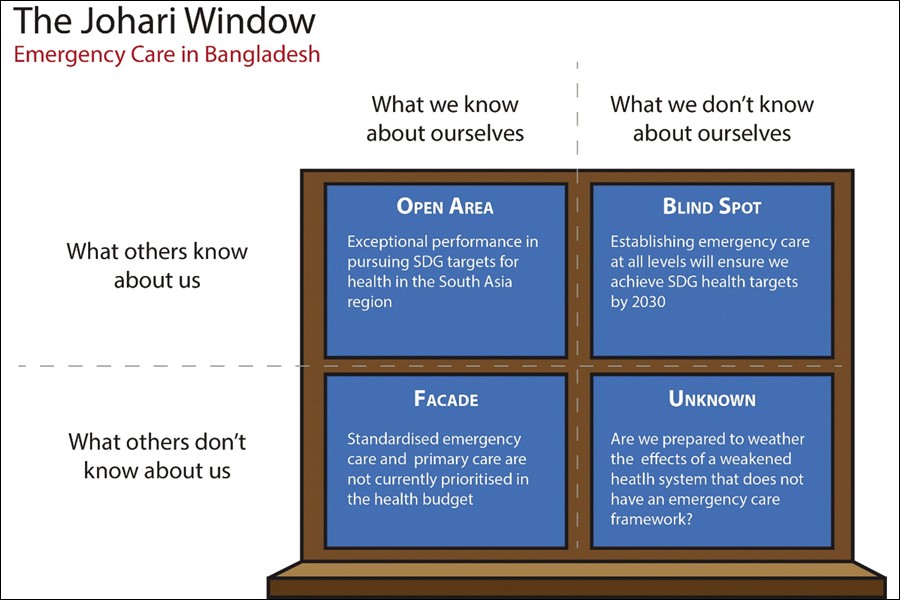
Mapped to the Johari Window of the known and the unknown, as illustrated below in Figure 1, emergency care (EC) remains firmly entrenched in a blind spot in Bangladesh. There have been many studies on the impact of the introduction of emergency care in low-and middle-income nations, but policymakers remained oblivious of the need. The World Health Organisation (WHO) has recognised this fact and realises that countries that have not established an EC Framework will fail to meet the Sustainable Development Goals (SDGs) in several criteria as set out by the United Nations Conference on Sustainable Development in 2012.
To this end, the WHO developed an Emergency Care Framework and also introduced a mandate in the 72nd World Health Assembly, held in 2019, for establishing EC systems as a major component of universal health coverage.
This is very important for Bangladesh and the evidence is plain to see. In the 1960s the under-5 mortality rate in Bangladesh was 247 per 1,000, and this dropped to 127 in 1992. With improved nutrition, vaccination programmes and other national health campaigns, the current rate is now down to 22 per 1,000. A drop of over 90 per cent in just over 60 years is remarkable, but it is unlikely that we will attain the lowest rate of 2.0 per 1,000 without introducing emergency care services for sepsis, drownings, road-traffic collisions and other types of trauma.
The lack of Emergency Medicine services will similarly be felt across targets like maternal and infant mortality, mortality from non-communicable diseases, road-traffic deaths and suicide rates, to name but a few. Leaving aside the social implications, the financial burden of such avoidable deaths is indeed immense.
Disability-adjusted life year (DALY) has been used as a time-based measure of the overall burden of disease, predominantly in low- to middle-income nations. It combines the years of life lost (YLL) due to premature mortality and years of life lost due to time lived in states of less-than-full health or in disability (YLD). This statistic works well with EC as it not only accounts for the death from emergency presentations but also the disabilities sustained due to sub-optimal care for presentations that are deemed time-critical.
Although no in-depth study has been conducted on the effects of emergency care in Bangladesh, gross data relating to DALY is available. The current crude death rate is 5.8 per 1.000 of the population, but this will include deaths upon which emergency care would have no impact. A 2010 estimate of people living with disability in Bangladesh puts the figures at 9.0 per cent of the entire population. And 27 per cent of these disabilities are physical, which may correlate to the failures of emergency care. The study recognised genetics, birth complications, maternal malnutrition, child malnutrition, incidences of particular diseases, lack of awareness, lack of early detection, lack of access to proper treatment, and poverty as causes of disability. Altogether, the economic impact of disability on Bangladesh was 1.74 per cent of its GDP.
Global studies estimate that the cost to avert a DALY in countries with medium Human Development Indices (Bangladesh has an HDI value of 0.661, ranking it at 129 out of 191 countries) is between USD 997 and USD 36,091 which stood at 0.67 per cent of GDP per capita on average. In low-HDI countries, this drops down to 0.34 per cent of the GDP, valued between USD 109 and USD 3507. It can thus be surmised that any intervention to avert a DALY that costs below 0.67 per cent of the GDP could be considered cost-effective.
Cost-effectiveness of a comprehensive rural acute care facility in Bangladesh was assessed by McCord et al in 2003, and the cost to avert one DALY was found to be USD 15. The acute care seen in this facility ranged from trauma, infectious diseases, acute abdomen and major surgical infections as well as maternal emergencies. These presentations align directly with standard emergency-care management. With the current per-capita GDP of Bangladesh being estimated at USD 2,847, the intervention at this facility to avert a DALY lies at 0.53 per cent.
Although the math is not exact, the evidence weighs in heavily. A failure to invest in an effective Emergency Care framework for Bangladesh immediately will not only cost us our SDG targets of 2030 but also will deprive the nation of the much-needed economic growth it needs to sustain the current plans of modernisation.
The writer is a specialist in international emergency medical care, working with the ZABS Foundation in Bangladesh and Doctors Worldwide in the UK. He is also a consultant in emergency medicine in the NHS, based in London.
dr.msahmad@gmail.com