Man-made disasters and earthquakes: Plan and action
M Rezaul Karim | Sunday, 9 March 2014
Bangladesh has a long history of major disasters and natural calamities. Millions of lives have been lost over the years. The medical backup required to save the victims was never up to the standard. Moreover, the facilities near a disaster incident had to take the maximum burden with available minimum regular resources. Rescue and salvage operations were never systematically planned and organised to face a chaos. However, over the last decades the country has shown major successes and developments in managing disasters.
Mass casualty incidents (MCI), emergencies and disasters frequently affect Bangladesh with widespread social, economic and public health consequences. Due to geographical location, Bangladesh has long been facing several devastating natural disasters and is prone to cyclones, tornadoes, flood, tidal wave, and even earthquakes. Apart from the regular flood, storms and cyclones, Bangladesh in the recent years has experienced a number of major natural and man-made disasters, such as landslide, building collapse, fire, terrorist attack etc. In addition, road traffic accidents, capsize of boats and launches have become regular occurrences in different areas of the country. All these disasters resulted in enormous human sufferings, with loss of lives, assets and productivity.
Disasters are not only bigger than other mishaps; they have a significant impact on the community, resources and institutions. We are required to respond to those. Some disasters may overwhelm the capacity of the hospitals/communities and their resources. Hence, adequate planning and training of health personnel is required if hospitals are to respond efficiently and effectively to disasters, especially to mass casualty incidents. Health personnel must be aware of the pattern of different types of injuries, which occur in different disasters, particularly in mass casualty incidents. Then they will be able to plan appropriate, minimal and timely interventions in MCIs.
Similarly, man-made disasters have become regular occurrences in the recent years causing significant impact in terms of physical, mental, social and economic losses. The population of the country is increasing gradually. Simultaneously, industrialisation, urbanisation, and internal migration of the people are also gaining faster speed.
Some recent casualties caused by unscrupulous people have resulted in deep concerns and worries in and abroad about the safety of people in their work places. On 24 April, 2013, Rana Plaza, an eight-storey commercial building with apparel factories, collapsed in Savar, near Dhaka, the capital of Bangladesh. The search for the dead ended on May13 with the death toll reaching 1,129. It is considered to be the deadliest garment factory accident in recent history, as well as one of the deadliest structural failures in modern times. The fire incident which took place at Nimtoli in Old Dhaka on June 3, 2010, was indeed another terrible disaster. In the devastating fire at Nimtoli, at least 117 people died and hundreds were injured, with many of them left in critical conditions. The devastating fire generated from unsafe storing of chemicals in a residential building, which was not constructed for this purpose, and there was no safety measures at the store, although storing of inflammable chemicals at residential locations is a punishable offence under the Acid Control Act. December 14, 2010 at least 28 garment workers died and dozens more have been injured when a fire broke out on the 9th and 10th floors of the "That's It Sportswear Ltd" factory just outside the capital Dhaka. On June 1, 2010 a five-storey building, poorly built on a small stretch of land no bigger than 15 feet by 12 feet, completely collapsed in the early hours of the day over another three-storey, tin-roofed house killing a 29 people including children. Forty-four schoolboys were killed and 15 others injured as a truck plunged into a roadside ditch near Abu Torab Bazzar at Borotakia of Mirsarai upazila in Chittagong on July 11, 2011.
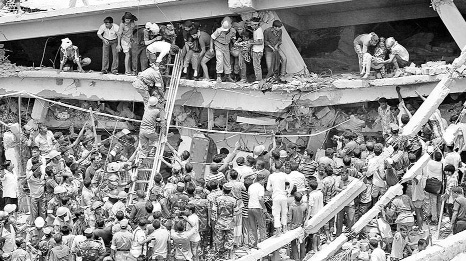
A number of incidents occurred in this decade that may be treated as major human-induced disasters. Some twenty people were killed and more than two hundred injured in a grenade attack on August 21, 2004.
The incident of grenade attack and the medical backup situation at Dhaka Medical College Hospital (DMCH) could be recalled as a 'turning-point' in the history of managing mass casualties in Bangladesh. After the deadly incident of grenade attack, people took no more than 10 minutes to rush the victims to DMCH, after the first injured was taken there. The relatives, party activists, law enforcers and journalists crowded the entrance to the Emergency Ward, as more injured were being taken there. Over 150 injured were taken first to the DMCH. The authorities moved the old patients of ward-32 to other wards and made beds on the floor but could not manage enough space for the injured. Most of the injured were, however, moved to other hospitals as the hospital could not accommodate them. A chaotic situation unfolded in the hospital compound. A long line of people stretched out to the mortuary and ward-32, where the injured were being treated, blocking the walkway. People chased the police out of the DMCH after they were deployed there at 6:10 pm to control the crowd. Police, however, were deployed again at 6:45 pm to clear the walkway to the mortuary and ward-32 and they clubbed the crowd twice. DMCH urged people to donate blood for the injured. Some 50 people crowded there, but the authorities had only 24 bags till 7:30 pm. The hospital did not have enough bags for the people who went there to donate blood.
This incident was an eye-opener to the policymakers, medical professionals, and disaster management experts. The Directorate of Health Services took up an initiative to launch the drive of "Mass Casualty Management (MCM)" in medical management under a HOPE project, supported by USAID. The guidelines on MCM have been developed for the hospitals at primary (upazila) and secondary (district) levels. At the same time, an international NGO, ActionAid, and European Commission came forward to work on MCM under the financial support of DIPECHO project.
As Mass Casualty Management is not broadly popular to the people of Bangladesh, it can be discussed in a few words. A mass casualty is any event, in which the number of victims is large enough to overwhelm available resource, disrupting normal emergency and healthcare services. An example can be placed here to explain it properly. Management of forty four injured patients might not be Mass Casualty for DMCH, but it was obviously Mass Casualty for Mirsarai upazila hospital on July 11, 2011, when forty-four schoolboys were killed and 15 others injured as a truck plunged into a roadside ditch.
The patients may be victims of any kind of disaster including earthquake, flood, fire, plane crash, terrorist attacks - bomb blast, biological weapon etc. Beside these trauma cases, the patients could also be victims of disease outbreaks like diarrhoea, dengue haemorrhagic fever or viral infection during floods etc. Therefore, it is a need for hospitals to be able to react rapidly and appropriately to disasters. So plans must be developed and tested and staff should be trained in order to achieve the desired goal. Planning must be there for the roles and responsibilities that a hospital may anticipate during such a situation. This will require hospitals to have their strong contingency planning with emphasis on 'surge capacity' as well as diversion policies, mutual aid arrangements with other hospitals. They must be prepared for prompt and efficacious management.
The concept of MCM includes Epidemiology of Disasters, Mass Casualty Incident (MCI), Hospital Contingency Plan, Hospital Emergency Incident Command System (HEICS), Triage, Integrated Emergency Medical Services (IEMS), Resuscitation and Emergency Care, Managing Resources and Public Relation, Medico Legal Aspect of Mass Casualty and Psychosocial care. The Triage and Golden Hour might be interesting to many. In this context, it can be discussed in brief.
Catastrophic disasters inevitably lead to large numbers of deaths and persons with injuries in the immediate aftermath. Many lives can be saved if patients are adequately and promptly managed. Major hospitals of Bangladesh are located in the two major cities - Dhaka and Chittagong. These two cities, including Sylhet, are at the high risk of earthquake owing to their location, densely populated nature and the profusion of multi-storey buildings. Industrialisation, unplanned urbanisation, and city-bound movement of the people are fast increasing in these cities. These lead to a favourable condition for increasing mishaps in the forms of road accident, building collapse, fire break-out etc. Inadequate precautionary measures at residential buildings, markets and shopping malls and industries, especially at garment factories, have raised the potential risk of fire disasters. Experts feel that the careless attitude of the drivers and vehicle and vessel owners is the main cause of frequent road and waterway accidents in Bangladesh. Construction of buildings, ignoring the National Building Code, is the major cause of building collapse.
Our healthcare infrastructure is one of the best in the region. We have a number of medical colleges; and one large district hospital in every district. Almost every upazila (sub-district) has one health complex. Many other government facilities are also providing healthcare services. Besides these, we have a strong private healthcare sector, which has been contributing a lot to meeting the daily healthcare needs. Even then, the capacities of the health institutions are sub-optimal to effectively deal with major disasters or emergencies.
It is true that major hospitals in Bangladesh have inadequate systems in place to handle mass casualties in case of a disaster. As a result of this inadequate system and capacity, most hospitals rely upon ad hoc decision making in the event of a disaster. Consequently, they fail to function properly during disasters, leading to unwanted deaths and suffering of the people. In this regard, a Hospital Contingency Plan needs to be in place. Its objective is to strengthen the emergency response operations of a hospital with a view to reducing the potential health effects of emergencies and disasters in an organised way.
Mock drills may be designed and organised with the objective of strengthening institutional capacity of the hospitals by preparing the hospital administrators, senior health officials and physicians working in the casualty and emergency departments, so that they are more skilled in taking rapid action in case of any mass casualty incident in order to provide as rapidly as possible the greatest benefit for the largest number of casualties. Another important objective of the mock drill is to find out how other stakeholders like the community volunteers can participate in mass casualty management during emergency.
Professor Roger Balham of Colorado State University first came up with his recent research findings that major earthquakes might take place in the sub-Himalayan region, including Bangladesh. Another study of Michigan University has pinpointed that Dhaka is one of the earthquake-vulnerable spots among the top cities because of its unplanned urbanisation. A strong earthquake of 8.6-magnitude occurred in Assam on August 15 in 1950, killing 1,526 people. Another 8.1-magnitude quake hit Assam on June 12 in 1897, killing 1,500 people. The casualties were less because of low density of population and fewer numbers of concrete structures at that time. But most of the concrete structures in Dhaka and Sylhet cities will be fully or partially damaged by a major earthquake.
Comprehensive Disaster Management Programme (CDMP) under the food and disaster management ministry conducted a study from February 2008 to August 2009. The study report reveals that some 78,323 buildings will be destroyed completely if a 6-magnitude earthquake shakes Dhaka originating from its beneath, causing havoc throughout the densely populated capital city. In case of a 7.5-magnitude earthquake originating from Madhupur Fault, the study says, some 72,316 buildings in the city will be damaged totally, while 53,166 partially, and will generate a total of 30 million tonnes of debris, killing some 131,029 people instantly and injuring 32,948 others. It says if an 8.5-magnitude of tremor from the plate boundary of Fault-2 hits the region, some 238,164 buildings will be destroyed completely across the country. Some 30 million tonnes of debris, equal to 2,880,000 truckloads (25 tonnes for per truck), will be generated if a 6-magnitude earthquake jolts the city from beneath it.
Although some initiatives on MCM have been taken and are being implemented by the Directorate of Health Services, still those are on ad hoc basis. It seems that the directorate has no concrete plan to enhance the capacities of hospitals at all levels to face any unpredictable incidents. The initiatives are being implemented under the financial support of an external agency's project. The major hospitals have developed contingency plans under the support of that project, but as there is no provision for reviewing the plans, they have not been put into effect. As per the contingency plan of Dhaka Medical College Hospital, temporary centres can be established if the hospital collapses fully or partially in an earthquake. But there is no detailed indication as to how it would be materialised in case of emergency. The guidelines for developing Hospital Contingency Plan and Mass Casualty Management Drill have been developed. But still it has not been approved by the ministry. And, there is no sign of materialising neither the plan nor the drill at all hospitals of the country. The directorate of health services has taken another initiative to develop the strategy of MCM. It might be a direction regarding materialising the capacities of the hospitals to cope with emergencies.
In Bhuj earthquake in 2001, a 44-year-old 250-bed civil hospital collapsed, killing some 150 patients-including several expectant mothers and their 25 relatives, 7 nurses, and 4 employees. The Bhachau area hospital was completely flattened. Operating theatre lights could be seen dangling out of the mass of debris that remained of the 50-bed hospital.
A 7.0 magnitude earthquake struck Haiti and devastated Port-au-Prince on January 12, 2010. Although the exact number was difficult to determine, the highest reliable death count was estimated at 220,000. Haitian government's estimate was higher. The Presidential palace, Parliament and many other important structures were destroyed, along with countless homes and businesses, leaving many homeless. Several hospitals have been seriously damaged and others are swamped by casualties. The main hospital in the hillside suburb of Petionville collapsed, and its 60-bed trauma centre in Port-au-Prince was seriously damaged.
Most of the buildings of Dhaka Medical College Hospital are century-old and the assessment of structural vulnerability has not been done yet. The minister of food and disaster management, after a tremor recently, expressed eagerness at a meeting that the assessment would be done immediately. Nobody knows what will happen if Dhaka or Chittagong or Sylhet experiences any severe situation.
The writer works as free-lance consultant on Disaster Management and Climate Change & Adaptation. rezaul.karimkm@gmail.com