 A healthcare outlet: Good health raises human capital levels. —FE Photo
A healthcare outlet: Good health raises human capital levels. —FE Photo ![]() In developing countries, nearly half the population suffers from multidimensional poverty with deprivations in health and other living conditions. It is the poor who suffer from ill-health, malnutrition, communicable and non-communicable diseases, lack basic amenities of healthcare, and, as a result, are not able to contribute effectively to the economic growth of a country.
In developing countries, nearly half the population suffers from multidimensional poverty with deprivations in health and other living conditions. It is the poor who suffer from ill-health, malnutrition, communicable and non-communicable diseases, lack basic amenities of healthcare, and, as a result, are not able to contribute effectively to the economic growth of a country.
Health has an important role in achieving sustainable economic growth. There exists a two-way relationship between health and economic growth. Improved health increases productivity of the labour force, and thus promotes economic growth. On the other hand, economic development leads to improvements in nutrition, better sanitation, innovations in medical technologies, all of which help increase the life expectancy and reduce the maternal, child and infant mortality rates.
According to the Goal 3 of the Sustainable Development Goals (SDGs), good health is a vital component of well-being. Good health increases human capital levels, which in turn enhances economic productivity of individuals and drives economic growth. A heathy workforce finds it easier to adopt new technologies, has low rates of absenteeism and helps raise output.
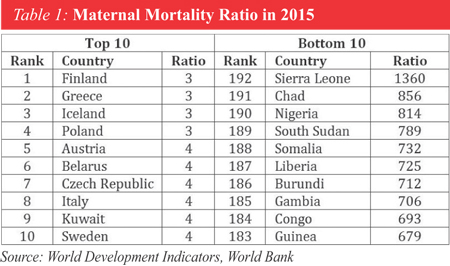
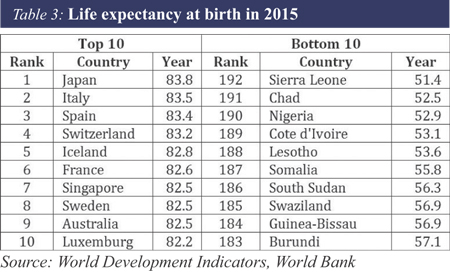
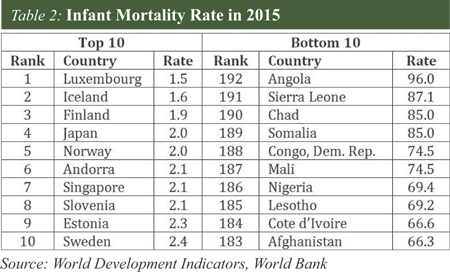 As maternal-mortality ratio, infant-mortality rate and life expectancy at birth are among the key indicators of health, we have ranked among the top and bottom 10 countries in terms of these indicators for the year 2015 using a sample of 192 countries (for which the data are available). Maternal-mortality ratio is the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births. Infant-mortality rate is the number of infants dying before reaching one year of age, per 1,000 live births in a given year. Finally, life expectancy at birth indicates the number of years a newborn infant would live if prevailing patterns of mortality at the time of its birth were to stay the same throughout its life. All data have been obtained from World Development Indicators of the World Bank.
As maternal-mortality ratio, infant-mortality rate and life expectancy at birth are among the key indicators of health, we have ranked among the top and bottom 10 countries in terms of these indicators for the year 2015 using a sample of 192 countries (for which the data are available). Maternal-mortality ratio is the number of women who die from pregnancy-related causes while pregnant or within 42 days of pregnancy termination per 100,000 live births. Infant-mortality rate is the number of infants dying before reaching one year of age, per 1,000 live births in a given year. Finally, life expectancy at birth indicates the number of years a newborn infant would live if prevailing patterns of mortality at the time of its birth were to stay the same throughout its life. All data have been obtained from World Development Indicators of the World Bank.
Table 1 shows that Finland, Greece, Iceland and Poland have the lowest maternal-mortality ratio of 3, whereas, Sierra Leone has the highest 1360. Nine out of the top 10 countries are from Europe. In contrast, all the bottom 10 countries are from Sub-Saharan Africa. However, the Goal 3 of the SDGs has set a target of reducing global maternal-mortality ratio to less than 70 by 2030. Table 2 depicts that Luxemburg is the leading country in terms of the lowest infant mortality rate (1.5) and Angola has the highest at 96. Eight out of the top 10 countries are from Europe, and again, 9 out of the 10 bottom countries are from Sub-Saharan Africa. The Goal 3 of SDGs provides for reducing infant mortality as low as 12 by 2030. Table 3 shows that Japan has the highest life expectancy of 84 years while Sierra Leone the lowest 51 years. Again, 8 out of the top 10 countries are from Europe, and all 10 bottom ones are from Sub-Saharan Africa. All these suggest that still a number of countries in the world have to make some dramatic progresses to achieve the targets of SDGs by 2030.
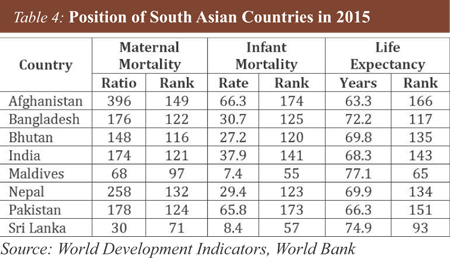
Table 4 illustrates the positions of the South Asian countries among those 192 countries in terms of the aforementioned health indicators. It is observed that both Sri Lanka and the Maldives are doing well in terms of all the three health indicators. In South Asia, the Maldives has the highest life expectancy of 77 years and the lowest infant-mortality rate of 7.4. Sri Lanka has the lowest maternal-mortality ratio of 30. In cases of infant mortality and life expectancy, Bangladesh performed better than India, Pakistan, Nepal, Bhutan and Afghanistan. Also, in the case of maternal mortality, Bangladesh performed better than Pakistan, Nepal, Bhutan and Afghanistan did. Afghanistan has the worst performance in all three indicators among the South Asian countries.
 In order to explore the relationship between economic growth and health a cross-country panel econometric analysis is conducted using a panel data of 192 countries for the years 1970-2016. In this analysis, the dependent variable of the model is the log of real gross domestic product (GDP). The explanatory variables are log of labour, log of capital stock and three health-related indicators (infant mortality rate, maternal mortality ratio, and public expenditure on health) in three separate regression models. All data, apart from the labour and capital stock, are from World Bank's World Development Indicators. The labour-and capital-stock data are obtained from Penn World Table 9.0. The fixed-effect panel-regression results suggest that coefficients of all three health-related indicators are statistically significant with expected signs. A 50-unit decline in infant-mortality rate is associated with the increase in real GDP by 1.0 per cent. Furthermore, 50-unit decline in maternal mortality is associated with the increase in real GDP by 0.01 per cent. Finally, a one-per cent increase in the real public health expenditure is associated with the rise in real GDP by 0.3 per cent.
In order to explore the relationship between economic growth and health a cross-country panel econometric analysis is conducted using a panel data of 192 countries for the years 1970-2016. In this analysis, the dependent variable of the model is the log of real gross domestic product (GDP). The explanatory variables are log of labour, log of capital stock and three health-related indicators (infant mortality rate, maternal mortality ratio, and public expenditure on health) in three separate regression models. All data, apart from the labour and capital stock, are from World Bank's World Development Indicators. The labour-and capital-stock data are obtained from Penn World Table 9.0. The fixed-effect panel-regression results suggest that coefficients of all three health-related indicators are statistically significant with expected signs. A 50-unit decline in infant-mortality rate is associated with the increase in real GDP by 1.0 per cent. Furthermore, 50-unit decline in maternal mortality is associated with the increase in real GDP by 0.01 per cent. Finally, a one-per cent increase in the real public health expenditure is associated with the rise in real GDP by 0.3 per cent.
It is thus observed that a country's collective health status affects the country's economic growth rate. Improvements in the health status of a nation has a positive impact on economic growth. Therefore, the health sector has to be included as a vital part of the development strategy of a country as illness and disease can act as strong barriers to economic growth. Investment in the health sector should be included as an important component of economic policy in order to sustain, and improve on, economic and social outcomes. Governments need to consider spending on healthcare as an investment and not a cost. Therefore, there is a need to raise the level of public health expenditure and its efficient uses. Without significant improvements in infant-mortality rate and maternal-mortality ratio, economic growth is bound to be constrained.
Dr. Selim Raihan, Professor, Department of Economics, University of Dhaka, & Executive Director, SANEM: selim.raihan@gmail.com
Sunera Saba Khan, Senior Research Associate, SANEM.
suneraecondu@gmail.com
© 2026 - All Rights with The Financial Express