![]() Would you be concerned, if you are told about an ancient disease that is so virulent in the present day that it actually makes the Covid-19 pandemic seem like a seasonal 'flu? What if you are told that this disease has already spread all across the globe and potentially into the space with every manned-mission? How about telling you that if we put it into figures and say that in the fifteen-year period to 2030 this disease will cost the world economy at least 1.8 trillion US dollars? If these statements do not grab our collective attention, then the risk we face from this disease is far greater than can be imagined.
Would you be concerned, if you are told about an ancient disease that is so virulent in the present day that it actually makes the Covid-19 pandemic seem like a seasonal 'flu? What if you are told that this disease has already spread all across the globe and potentially into the space with every manned-mission? How about telling you that if we put it into figures and say that in the fifteen-year period to 2030 this disease will cost the world economy at least 1.8 trillion US dollars? If these statements do not grab our collective attention, then the risk we face from this disease is far greater than can be imagined.
Almost 8.0 per cent of all deaths globally can be attributed to it with an estimated 4.4 million people dying from it every year. This equates to over 12,000 deaths daily in comparison to the 5,000 daily deaths due to the Covid-19 till date. Even the in-flight medical events log for U.S Astronauts during the Space Shuttle Programme (from April 1981 to January 1998) found this to account for 7.6 per cent of all diseases that occurred in space.
The disease that is being referred to is a traumatic injury, both unintentional and violence-related. There is a high likelihood that the newspaper you are reading has already relegated reports of yesterday's deaths from trauma to the inside pages. Despite the work of activists and organisations, we have become so desensitised to mortality from trauma that we do not even register them unless a mass casualty incident occurs, and that too, if it only happens at our doorsteps.
Most traumatic injuries occur because of road traffic crashes, falls, and acts of violence against oneself or others. These mechanisms essentially cause a destructive effect on skin, bones, muscle and other soft tissue by transferring mechanical energy. Traumatic injuries also occur when heat or chemical energy is transferred to the body to cause damage, such as in the case of burns, poisoning and drowning. It should therefore be no surprise that traumatic injury is the leading cause of death during the first four decades of life, at a time in our lives when we are the most active.
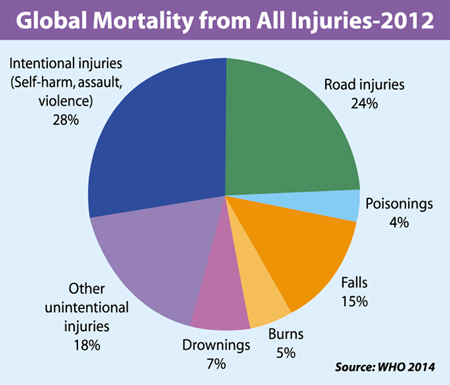
When we start to peel back the layers of trauma, we can see that road traffic injuries account for approximately 1.35 million deaths worldwide. This is equivalent to 3,700 people dying daily and almost 25.0 per cent of the total burden. Numerous exercises in cost analysis have shown the immediate impact of road traffic collisions on the economy is quite extensive, costing nations anywhere between 20 and 40 per cent of their gross domestic product (GDP). In a developed health economy, only 2.0 per cent of costs are spent on direct healthcare needs, such as transportation to the hospital, emergency visits and stay in hospital. Over 87.5 per cent of the costs are required to cover for police, insurance administration and damage to property. The remaining 10.0 per cent or so of costs are indirect costs such as wages lost due to hospitalisation and mortality (which includes years of potential life lost, and deaths). In a developing healthcare economy like Bangladesh, direct costs amount to about 80.0 per cent of total costs while 20.0 per cent remain indirect. Even though the distribution of cost is relatively well balanced between the two differing systems, it should be noted that Bangladesh remains an 'out-of-pocket' health economy and a single episode of traumatic injury can cost over 80.0 per cent of a family's monthly income. It should also be noted that the age groups most likely to be affected by trauma are the 25 to 44 years old and the 45 to 64 years old, both groups contributing the most to economic productivity.
Unfortunately, the cost of trauma does not stop there. Following these immediate expenses, there are long-term consequences and costs associated with trauma. For the majority of patients who do not succumb to their traumatic injuries, there is the ongoing need for rehabilitation, which is required to bring them back to their pre-injury productivity. A failure of rehabilitation will result in increased disability-adjusted life years (DALY) which can be expressed as a cost incurred due to the number of years lost due to ill-health or disability.
Leaving aside the death and injury, exposure to any form of trauma can increase the risk of mental illness, particularly in childhood. Trauma can push a family into poverty, and that can lead to cycles of crime and violence. The stress resulting from trauma can lead to smoking, alcohol and substance abuse. It can trigger chronic diseases like heart disease, diabetes and cancer. When we take all of this into consideration, the financial impact of trauma rises exponentially, and all previous estimates we have made thus far start to look quite conservative.
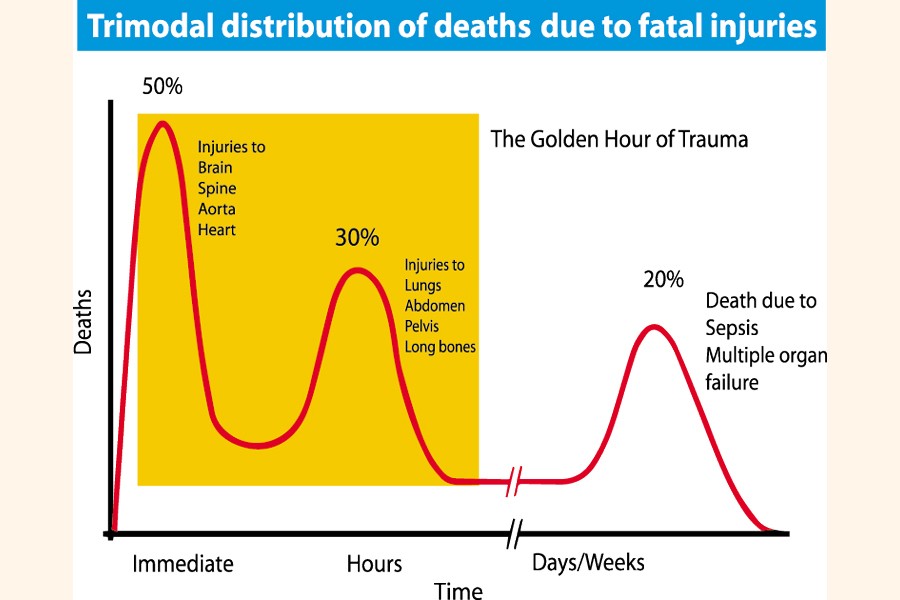
So, is all hope lost, or can we recover from this seemingly insurmountable burden? With improvements made in science and technology, there are an increasing number of treatment procedures that are being made available to the trauma patient. One such procedure, of many, is REBOA or Resuscitative Endovascular Balloon Occlusion of the Aorta. In a scenario where a patient has sustained a major injury to the abdomen, or the region below, and is actively losing blood by haemorrhage, it is highly unlikely that such a patient will survive a prolonged journey to a centre of definitive care, where bleeding vessels can be repaired in a theatre setting by an experienced vascular surgeon. These patients usually constitute the first and highest peak of immediate deaths in the tri-modal distribution of death due to fatal injuries. REBOA increases the chance of survival of these patients by placing a medical balloon into the main artery of the body (aorta) and stopping blood loss. This can be done out in the field at the accident site, or at a local hospital 'pit-stop' to allow for resuscitation before moving to the definitive centre.
For us in Bangladesh, this cutting-edge technology may seem to be out of place due to the costs associated with materials and training. It may be something that could be considered when the country's trauma services are strengthened, but there is no place for it now, in the current setting. However, there are many simpler procedures that can currently be done that will have an impact on the very same group of patients. Simple burr-hole procedures to decrease the pressure in the skull caused by a build-up of blood resulting from a head injury can buy precious time and prevent secondary injuries to the brain tissue. Again, this can be done locally at very little cost, while the definitive brain surgery can be done at a more distant site.
To strengthen trauma services nationally, all hospitals must have a working emergency care unit that is trained in the medical management of trauma, thus allowing these patients to be resuscitated as best possible, before they undergo operative procedures classed as damage control surgery. Further, as already evidenced by multiple health systems, trauma care resources are best set up into a trauma network of hospitals where there is a central major trauma centre that hosts, and is supported by, satellite hospitals acting as trauma units. Patients can thus by-pass their local hospitals and head to the major trauma centres, if the presentation is urgent or may pit-stop at the local hospital for resuscitation, before being moved on to the centre.
 A functioning trauma network is designed to provide the best possible outcome for the early and late death peaks of the tri-modal distribution. However, the key to relieve the financial burden that trauma places on the economy is by reducing the immediate deaths. This can only be done by the prevention of trauma in the first place; and injury and violence can be prevented because they are both predictable. In our present context, it can easily be predicted that if things continue to run the way they are on the newly-opened elevated expressway, serious accidents will take place as drivers are neither keeping to the designated speed limits nor they are trained on the rules of mass transit driving. Regulations must be applied early and enforced rigorously, otherwise the price we pay will be severe.
A functioning trauma network is designed to provide the best possible outcome for the early and late death peaks of the tri-modal distribution. However, the key to relieve the financial burden that trauma places on the economy is by reducing the immediate deaths. This can only be done by the prevention of trauma in the first place; and injury and violence can be prevented because they are both predictable. In our present context, it can easily be predicted that if things continue to run the way they are on the newly-opened elevated expressway, serious accidents will take place as drivers are neither keeping to the designated speed limits nor they are trained on the rules of mass transit driving. Regulations must be applied early and enforced rigorously, otherwise the price we pay will be severe.
Anecdotes aside, there is compelling scientific evidence that demonstrates the value of injury prevention. Investing USD 1 for every smoke detector to prevent fires saves an economy USD 65 in return. A similar investment in child restraints and bicycle helmets can save USD 29. Studies in Bangladesh itself have shown that teaching school-aged children swimming and rescue skills can help save USD 3,000 per death. The age-old adage 'prevention is better than cure' truly does stand the test of time when we see that an estimated 10.0 per cent reduction in adverse childhood experiences could account for an annual saving of USD 105 billion in Europe and North America.
Some may not consider injuries a disease in the true sense of the word, and some may not consider it a pandemic. However, the fact remains that traumatic injuries, both inflicted and unintentional, place a substantial burden upon health economies across the world. Trauma research and care still remain an under-funded and under-represented medical field. If we continue to neglect the impact of trauma, we will no longer be able to address the scale of this problem and risk perpetuating enormous human and financial costs.
Dr Mir Saaduddin Ahmad is a specialist in international emergency medical care, working with the ZABS Foundation in Bangladesh and Doctors Worldwide in the UK. He is also a consultant in emergency medicine in the NHS, based in London.
dr.msahmad@gmail.com
© 2026 - All Rights with The Financial Express