![]() Over the past five decades, Bangladesh has made significant progress in a number of important health sector areas. Maternal mortality rate has come down by almost two-thirds, and infant and child mortality rates were reduced by 44 per cent and 35 per cent respectively; Bangladesh's total fertility rate is currently approaching replacement level and is the lowest in South Asia (except for Sri Lanka). A number of diseases have either been eradicated or brought under control, e.g., smallpox, malaria and diarrhoeal diseases; blindness prevention has been reduced by 35 per cent. With the mainstreaming of nutrition interventions in the public sector, growing agricultural self-sufficiency and supportive policies, wasting among children has been brought down by half, while stunting and underweight prevalence have also come down to some extent. Earlier, Bangladesh met many of the health-related MDG targets including in areas of water and sanitation.
Over the past five decades, Bangladesh has made significant progress in a number of important health sector areas. Maternal mortality rate has come down by almost two-thirds, and infant and child mortality rates were reduced by 44 per cent and 35 per cent respectively; Bangladesh's total fertility rate is currently approaching replacement level and is the lowest in South Asia (except for Sri Lanka). A number of diseases have either been eradicated or brought under control, e.g., smallpox, malaria and diarrhoeal diseases; blindness prevention has been reduced by 35 per cent. With the mainstreaming of nutrition interventions in the public sector, growing agricultural self-sufficiency and supportive policies, wasting among children has been brought down by half, while stunting and underweight prevalence have also come down to some extent. Earlier, Bangladesh met many of the health-related MDG targets including in areas of water and sanitation.
A number of factors have contributed to the aforementioned achievements: timely policies, low-cost solutions, large-scale and innovative public health interventions, engagement of NGOs as delivery agents, use of technology and active involvement of the private sector in health service delivery, to name only a few. However, presumably, the low-hanging fruits have already been reaped, and the country now faces the challenges of covering the last mile and ensuring the quality of health-related service delivery.
The 'last mile' and quality assurance are, in all likelihood, going to be uphill tasks. Besides issues and challenges that are internal to the health sector, the ecosystem within which the sector operates has emerged as a key concern, plagued by a number of problems including a lack of good governance, growing inequities and rising inequality, a poverty rate which still stands at about 18 per cent and stressed macro-economic environment following the Covid pandemic and the war in Ukraine.
Bangladesh has a pluralistic and fragmented structure in the delivery of health services where public and private facilities, formal and informal service providers, and rural and urban health systems, exist simultaneously, without formal interfacing and defined point of accountability. The current health structure and health system have evolved during a time when the country's population was predominantly rural, the literacy rate was low and financial affordability was rather limited. Against this backdrop, a multi-tier rural-based health infrastructure was put into place supported by an extensive doorstep delivery of services and information. However, times have changed and it is now important to think about introducing universal health coverage (UHC) in line with the SDGs (Goal 3) and Bangladesh's aspiration to be a developed country by 2041.
The UHC envisages that all people have access to the full range of quality health services they need, when and where they need those, without being impeded by financial and other obstacles. Here there are many challenges though: rapid rural-to-urban migration, changing disease patterns, changing needs and expectations of patients/clients as a result of increased economic capacity and lifestyle changes and needs, a burgeoning private sector primarily motivated by profit and a host of other social, economic, climatological and geographical factors. These are pressing challenges that stand in the way of achieving UHC through the prevailing health sector system. Achieving the ambitious goal of UHC by 2030 is indeed going to be a formidable challenge in view of the limited time span to the target timeline, resource constraints and the complexity of the issues that will need to be addressed. Consequently, hard choices will have to be made. Against this backdrop, programmes targeting the most vulnerable with the highest impact will need to be prioritised in sequencing the actions to be taken.
The current paper has been developed as a policy brief on the basis of existing knowledge, literature review and expert opinion, and aims to review the relevant issues and identify the challenges and opportunities. It puts forward a set of concrete proposals to attain UHC in Bangladesh in alignment with SDG 3.
 Two critically important issues at present stand as major barriers to achieving UHC: the issue of out-of-pocket (OOP) expenditure and addressing the needs of the left behind communities.
Two critically important issues at present stand as major barriers to achieving UHC: the issue of out-of-pocket (OOP) expenditure and addressing the needs of the left behind communities.
The largest chunk of total health expenditure (THE) in Bangladesh is financed by OOP expenditure which rose from 55 per cent in 1997 to 67 per cent at present. According to the National Health Account Database of the WHO, OOP expenditure is defined as any direct outlay of households, including gratuities and in-kind payments, paid to health practitioners and suppliers of pharmaceuticals, therapeutic appliances and other goods and services, whose primary intent is to contribute to the restoration or enhancement of the health status of individuals or population groups. In practice, OOP is a part of private health expenditure. To put it in perspective, Bangladesh's high OOP expenditure compares quite unfavourably with the global average of 32 per cent and is highest in South Asia.
The largest share of OOP expenditure in Bangladesh is on medicine (64 per cent), followed by hospital services (14 per cent) and diagnostics (8 per cent). This significantly large amount creates financial stress and distress for about 9 per cent of households in Bangladesh; this is four times higher for the poorest households compared to the richest ones. Indeed, this scenario somewhat takes the shine off the country's poverty alleviation successes of the last three decades. If several other expenditures associated with accessing health services that are not captured by the survey are added, including money spent on e.g., transportation, accommodation, communication, food etc. of the patient and caregiver(s), the actual financial burden would be much bigger. As a matter of fact, the 2016 household survey data reveal that 4.5 per cent of the population (8.61 million people) fell into poverty because of high health-related expenditures (Sayem Ahmed et al, International Health, Volume 14, Issue 1, January 2022, Pages 84-96).
As is well known, a core element of the SDG agenda is to 'leave no one behind'. This concept envisages "a world of universal respect for equality and non-discrimination" between and within countries, including gender equality, by reaffirming the responsibilities of all States to "respect, protect and promote human rights, without distinction of any kind". A core aspect of ensuring equality is concerned with ensuring access to quality health services for all, without exception. Against this backdrop, the SDG agenda invokes the challenge of reaching the marginalised, vulnerable, and excluded groups and addressing the many facets of marginalisation, and vulnerability exclusion. The Centre for Policy Dialogue (CPD) in a 2017 study identified thirteen facets of marginalisation: income, gender, geographic location, life cycle, civil identity, disability, education and skills, health, occupation, religion and ethnicity, sexual orientation and shock-induced vulnerability (Quest for Inclusive Transformation of Bangladesh- Who Not to Be Left Behind; Citizen's Platform for SDGs, Bangladesh; Centre for Policy Dialogue; Dec 2017).
Taking the above into account, and in view of providing the necessary health care services, there is an urgent need to prioritise the needs of women and children, along with people living in hard-to-reach and climate-affected areas (haor, chars, coastal areas), indigenous communities (CHT residents, Santals, Garos, tea estate workers), slum dwellers, people living with disabilities including mental health disabilities, LGBTQ and religiously ostracised groups (e.g., Dalits). In addition to these groups, a growing number of workers also constitute vulnerable groups at risk of exclusion due to their work environment and the labour market scenario in Bangladesh- men and women and young boys and girls belonging to the workforce in factories and establishments in the formal (e.g., garments) and informal sectors (e.g., households, restaurants, car garages, micro-enterprises) and in hazardous industries (e.g., ship breaking, lathe machines). Health-related needs of these groups also demand attention.
ISSUES IMPEDING ACHIEVEMENT OF UHC: In order to address the important but complex issues of reducing OOP and leaving no one behind, several key health sector-related challenges will need to be adequately addressed. These include the following:
Drug pricing and availability. Drugs account for 64 per cent of OOP expenditure. No doubt, the drug policy of 1982 contributed in a significant way by instilling some discipline in the pharmaceutical market, through the introduction of an essential medicines list, banning combination drugs and encouraging and incentivising local manufacturing activities, to name only a few. Regrettably, following the 2005 and 2016 revisions, the policy has become more subservient to the business and commercial interests. This is manifested in the scaling down of the number of essential drugs, withdrawal of restrictions on combination drugs which are sometimes even ten times more expensive, inclusion of pharmaceutical representatives in drug policy review and allowing pharmaceutical companies to fix 'rational' MRPs for drugs instead of the mark-up based formula adopted in view of the 1982 drug policy. In June 2022, DGDA hiked the prices of 53 essential drugs; the prices of two commonly used drugs- paracetamol and metronidazole-increased by almost 70 per cent. Although not as highly priced as in some of the developed countries, given the high share of OOP expenses on drugs, the impact of such drug price rationalisation was likely to have a significant adverse impact on the availability of affordable treatment in Bangladesh.
Bangladesh meets 97 per cent of its needs for drugs through domestic production. However, about 90 per cent of the active pharmaceutical ingredients (API) have to be imported, mainly from two countries, China and India. The dependence on the import of APIs increases production costs and makes the industry vulnerable to supply shocks, as happened during the Covid pandemic. An industrial park for the production of active ingredients was set up a decade ago but is yet to be functional. A fully functional API park would allow local pharmaceutical companies to source at least half of their needs locally, bringing down the costs of drug production and thereby retail prices significantly. The earliest operationalisation of the API park demands priority attention on the part of policymakers.
While drugs are distributed free of cost from public health facilities, there are indirect costs to be paid, e.g., transport costs for coming to the centre, lost earnings etc. Also, while availability has increased in recent times, anecdotal information indicates that these facilities run out of supply after the first couple of weeks of the month. Powerful individuals exert influence and get drugs from these facilities by depriving others, particularly given the limited supply. Drugs not included in the essential medicines list have to be purchased from private facilities. Private pharmacies are doing a brisk business selling over-the-counter (OTC) and prescription drugs. The nexus between doctors, pharmaceutical companies and private diagnostic facilities, often through aggressive marketing practices including payment of commissions, is widely known.
Health needs of vulnerable groups. Bangladesh has quite a sophisticated and elaborate multi-tier health infrastructure in rural areas. In contrast, the urban scenario is rather disorganised. A modest network of primary health care centres run by NGOs through a project administered by the Ministry of Local Government, Rural Development and Cooperatives Ministry, along with a few dispensaries of the Ministry of Health and Family Welfare, are the main public sector facilities in urban areas. A thriving private sector which includes pharmacies, private clinics, diagnostic centres and hospitals and private practitioners fills the gap, providing services of varying quality at relatively high cost. Informal providers with dubious training and experience are also part of this provider system. However, oversight, accountability and control over their prescribing practices are rather weak.
Barring those living in hard-to-reach and climate-affected areas, or the indigenous population groups, a large part of the vulnerable groups mentioned earlier reside in cities, for the most part in slums which constitute 35 per cent of the population of the cities. Due to a host of reasons, these people are not able to access affordable health-related services. In the hard-to-reach and climate-affected regions and among indigenous and marginalised groups such as the dalits, tea garden workers and gipsies (bedes) who are scattered across the country, accessing services from health centres remains a challenge. Geographical factors matter as well as social standing and the stigma they often experience in receiving services from health facilities. Those with physical and mental challenges face additional difficulties. Health facilities are often not disability-friendly.
Lack of regulation, accountability and governance. Institutions vested with the responsibility of enforcing and overseeing health-related regulations have, due to lack of resources and leadership, failed so far to play their due role. The adverse results of this can often be seen in the way the private health sector functions: patients and their families are exploited financially, wrong treatment is meted out without accountability, medicines are over-prescribed and unnecessary investigations are advised. In the public sector as well, where government doctors often cross over to the private sector for private practice, clients are referred to private practice and private institutions, increasing costs and creating inconvenience. Licensing of private sector facilities is fractured, with DGHS hamstrung by a lack of adequate human resources and efficient systems to carry out the mandated tasks. The Medical Practice and Private Clinics and Laboratories Ordinance, promulgated in 1982, has not been reviewed since; many provisions have become obsolete in the backdrop of significant changes in the way health services are currently provided. Half-hearted instructions by various government agencies at different times have had little or no effect in raising the efficacy and performance of the health sector. Many of these facilities tend to cut corners to drive profit and compromise with quality. Several high court orders with directives to set prices for specific services and for the constitution of committees to draft various regulations are yet to be complied with.
Culture of nexus and kickbacks. Breaking the unholy alliance between the doctors on the one hand, and diagnostic facilities, pharmaceutical companies and hospitals on the other, would have a highly significant positive impact on the price patients pay for drugs and diagnostic tests. Commissions doctors receive for referring pathological tests are estimated to be as high as 40 per cent of total prescription costs. If this commission did not have to be paid, the prices of diagnostic tests would have come down significantly. The same is the case for medicines and hospital referrals.
Sub-optimal efficiency and lack of quality of care in facilities. Very few public health centres work at full capacity. Health facilities are not able to deliver the expected services because of a lack of trained and skilled providers. Often this is because vacancies are not filled and doctors and health staff are absent. These problems are further accentuated by the absence of appropriate facilities and equipment, lack of adequate and smooth supply of drugs and dismissive and disrespectful attitude towards patients. Other problems include a lack of hygienic conditions and long waiting times. Health service seekers from marginalised communities suffer the most. Consequently, people are discouraged from going to public health facilities.
Health centres sometimes refuse to take in and treat serious patients, apprehensive of the risk of reprisal from relatives and the local community if something goes wrong. Victims of road traffic accidents, for example, or delivery patients arriving with signs of eclampsia or haemorrhage, are often referred away, sometimes even without stabilising the patient. This sometimes proves fatal, increasing costs and creating serious inconvenience for the patient.
Against this backdrop, getting the public sector hospitals to work at full capacity and render the full range of mandated services has emerged as an urgent task. This is necessary to help more people to get treatment in public health facilities near where they live, this will also reduce OOP expenses.
Lack of local-level accountability. In the public sector, the lines of accountability are clearly laid out with the tiered health structure; linkages of this structure with the administrative wings of the government, including local government representatives are also spelt out clearly. While the the institutional and routine aspects of the accountability structure work to some extent (e.g. holding of various coordination meetings, reporting, flow of logistics etc.), the effectiveness of the present system in terms of protecting patients' interest, tackling absenteeism, maintenance of facilities at community clinics and upkeep of equipment etc tends to fall through the crack. Absenteeism remains a particularly difficult issue and a cause for concern. It can be traced to structural issues in the health system, a mismatch between working conditions and aspirations and career goals of health professionals and their socio-political networks. Those having influence, power and access to higher authorities can afford to be absent for long periods, overburdening and de-motivating their colleagues who lack connection and thus have to remain present at the clinics and facilities.
Community Support Groups for the Community Clinics and Hospital Management Committees at the upazila and district levels headed by the MP could have played an important oversight role in ensuring that public health facilities work effectively. However, sadly enough, these are either totally inactive or do not take their responsibilities with due seriousness. As regards the private sector, regulations to ensure accountability to patients and clients are very weak.
RECOMMENDATIONS: Against the backdrop of the above discussion, the following recommendations are proposed to reduce OOP expenses and address the healthcare needs of the vulnerable groups:
MAKE QUALITY DRUGS AFFORDABLE FOR ALL, ESPECIALLY FOR THE POOR AND VULNERABLE: Review and expand the essential drugs list. The 1980 National Drug Policy listed 150 drugs as essential. However, in 1995, the government issued a special communique listing only 117 drugs as essential. The 2016 revision of the National Drug Policy listed 285 essential drugs. The list is considered to be inadequate as it includes only 37 out of 309 drugs required for the treatment of non-communicable diseases (NCDs). The list ought to be updated on a regular basis through review and revision every two years, as suggested by the WHO. The range of essential drugs whose prices can be actively controlled by the government should be enhanced.
Reduce prices of other drugs. Since drugs constitute 64 per cent of OOP expenses, there is a need to reduce and control the price of drugs by revisiting the drug pricing policy and by enforcing strict monitoring of price.
Accelerate the production of active ingredients in-country. This is essential to reduce reliance on imports and to help bring down prices of locally produced medicines. This will also help avoid supply system disruptions.
Put in place a modern drug stock management system on an urgent basis. A national IT-based centralised drug-stock management system will ensure that health facilities get the required amount of drug supply in time and these could be distributed smoothly by maintaining the required quality of drugs. This will help monitor the availability of drugs and other health commodities, forestall drug shortages and stock-outs, improve drug storage, track inventory, and strengthen stock management.
TAKE SPECIAL MEASURES TO ADDRESS THE HEALTHCARE NEEDS OF VULNERABLE GROUPS: Undertake specific interventions for marginalised communities and those living in hard-to-reach areas. The government needs to team up with NGOs/CSOs to make services accessible to these groups by addressing the barriers mentioned in the previous section. Towards this, there is a need to deploy innovative methods to take health services closer to these communities (e.g., through telemedicine, and satellite/mobile clinics). Travel of needy people to service-providing centres ought to be facilitated (e.g., by providing transport services such as water ambulances). There are a number of interventions that have been successfully introduced by the country's NGO sector which the government can learn from. Resources should be deployed for their replication in public health service delivery.
In phases, make all service facilities disability-friendly. In spite of repeated commitments by the government, most public facilities continue to remain without proper disability access; such access is even more limited in private-sector health facilities. The government must make it a priority to install at least the minimum facilities such as ramps, disability-friendly receptions and toilets in all public health facilities. This should be made a mandatory requirement for issuing licences and renewal of licences for private facilities.
Introduce prepaid cards for households below the national poverty line. In view of this, the experience can be borrowed from the two types of prepaid cards under the Ayushman Bharat - Pradhan Mantri Jan Aarogya Yojana (PMJAY) and ABHA schemes introduced by the Indian government which allow low-income people to access services from empanelled facilities. Having a front-loaded card, with a reasonable amount of money, for all those included in e.g., the VGF or other social protection/safety net schemes will help address emergency situations when people belonging to disadvantaged communities face emergency health issues or experience chronic illnesses.
Right to Health Law. Although the Bangladesh Constitution pledges the right to life and protection of health, there are no specific laws to enforce these pledges. Lessons learned during the COVID-19 pandemic brought to the surface the urgent need for this. While there may be issues with the enforcement of such a law, its enactment itself will provide the disadvantaged people at least the legal means to claim their rights (similar to the case with the Right to Information Act 2009).
Minimum benefit package. Introduce a minimum benefit package for all with the condition to first seek health services from the Upazila Health Complex. This will act as a referral system for further and more advanced treatment.
Shasthyo Shurokhsha Karmasuchi. Undertake a thorough review of 'Shasthyo Shurokhsha Karmasuchi (SSK)' to examine the feasibility of its phase-wise expansion following necessary changes.
IMPROVE REGULATION, ACCOUNTABILITY AND GOVERNANCE BY STRENGTHENING INSTITUTIONS: Review, modernise and implement the 1982 Private Practice and Private Clinics and Laboratories Regulation Ordinance. The 1982 Ordinance has become redundant given that it was promulgated more than four decades back. No doubt, the healthcare sector has undergone a phenomenal transformation over these past years. The government needs to review and revise this Ordinance to come up with an appropriate framework as per which the private health sector can both function effectively and be held accountable. Steps must be taken to ensure proper enforcement of the provisions of the revised Ordinance.
Strengthen the jurisdiction and capacity of regulatory bodies. Government regulatory bodies e.g., DGHS, DGFP, BMDC and DGDA need to be strengthened in terms of staff capacity, automation and digitisation, financial resources, adequate logistical support and introduction of new ways of doing business. These are required to strengthen the capacity of these institutions to successfully perform the full range of activities they are mandated to carry out.
Create a National Health Authority to oversee the quality of healthcare. A high-level committee at the MOHFW level, with jurisdiction to work inter-ministerially, needs to be established to ensure standard quality of health care across public and private sectors. Various tools may be deployed towards this including accreditation, monitoring visits and regulation of technical as well as ethical aspects to improve the quality of care giving. The committee will work to progressively implement the 'Right to Health'.
BREAK THE CULTURE OF NEXUS AND KICKBACKS BY STRENGTHENING GOVERNANCE: Prepare specific guidelines for the ethical promotion of drugs and diagnostics. A set of strict guidelines is needed either as a corollary to the 2016 National Drug Policy or as a standalone government directive to regulate the marketing of drugs and promotional benefits and kickbacks given to prescribers and service providers by pharmaceutical companies and diagnostic laboratories. A monitoring system supported by the GRS system of the DGHS should be put in place to collect information and investigate patient complaints as regards overcharging. Improving overall governance of the health sector has emerged as a priority that needs to be addressed.
MAXIMISE EFFICIENCY AND EFFECTIVENESS OF SERVICE DELIVERY IN PUBLIC HEALTH FACILITIES: Take steps so that all public health facilities work at full capacity. Filling up all vacant positions and adequate provision of drug supplies and medical equipment are crucial to making a wide range of health care available to a larger number of people at their doorsteps. This in turn will bring down OOP expenses for the patients and reduce the harassment and hassles of going to distant places for treatment.
Manage waiting time. Long waiting time (long queues at various public health facilities) is a major deterrent that discourages people from accessing services from public health facilities. To reduce this, demand for the various services must be reliably estimated, and adequate human resources and a system of support, including logistics and supplies, must be ensured.
Address behavioural issues. More respectful behaviour on the part of health service providers will lead to patients being empowered to seek and get the services they need. This involves a significant cultural change, the foundation of which needs to be established during the education and training of various categories of health service providers. Behavioural aspects must be monitored, assessed and overseen during the working life of all health workers.
Build model pharmacies. The government should take the initiative to establish more model pharmacies across the country to ensure consistent supply and required quality of drugs. Gradually all pharmacies and drug stores should be brought under the DGDA enlistment. Model pharmacies should have trained graduate pharmacists in attendance.
ESTABLISH LOCAL-LEVEL ACCOUNTABILITY OF HEALTH SERVICE DELIVERY: Activate all local-level communities without delay. Community Clinic Groups, Community Clinic Support Groups, Union Family Planning Committees and MP-headed Upazila Health Management Committees are well positioned to support health service delivery at respective local levels. These can also hold the service providers accountable to the local communities. As it happens, currently these committees remain either non-functional or only occasionally functional. These committees must be activated without delay through proper government directives, by putting in place standard operating procedures. These bodies must provide oversight of the work of health facilities at the local level and address locally solvable problems. Their work needs to be supported.
Capture and act upon client feedback. At present, there is no system in place to capture client feedback. CSOs/NGOs should set up platforms for service users which would give voice to the service receivers. Such platforms could help bridge the attendant gaps in communication. Some allocations on the part of the government can help establish and promote such local platforms.
CONCLUDING OBSERVATIONS: Although ensuring UHC by 2030 appears to be an uphill task for a country with such formidable challenges facing its health sector, specific steps as outlined above could bring in significant positive changes. Three issues are important against this backdrop: political will to bring about the expected changes; adequate budgetary provisions to underwrite expenses; and the government's willingness to collaborate with non-state actors in the delivery of quality health services to the needy. GO-non-state sector partnerships could also be an effective tool to break the unholy nexus involving bureaucracy, private clinics, and diagnostic centres and health service providers. No doubt, it is difficult to generate political will without a strong commitment from the leadership of political parties. Commitments made by political parties in their respective election manifestos will help to generate the required political will, and hopefully drive concrete actions when the party is in power. Political commitment is also necessary to overcome the entrenched interests of health professionals and vested groups in the health sector who are also important vote banks and tend to wield substantial power and influence through their respective associations.
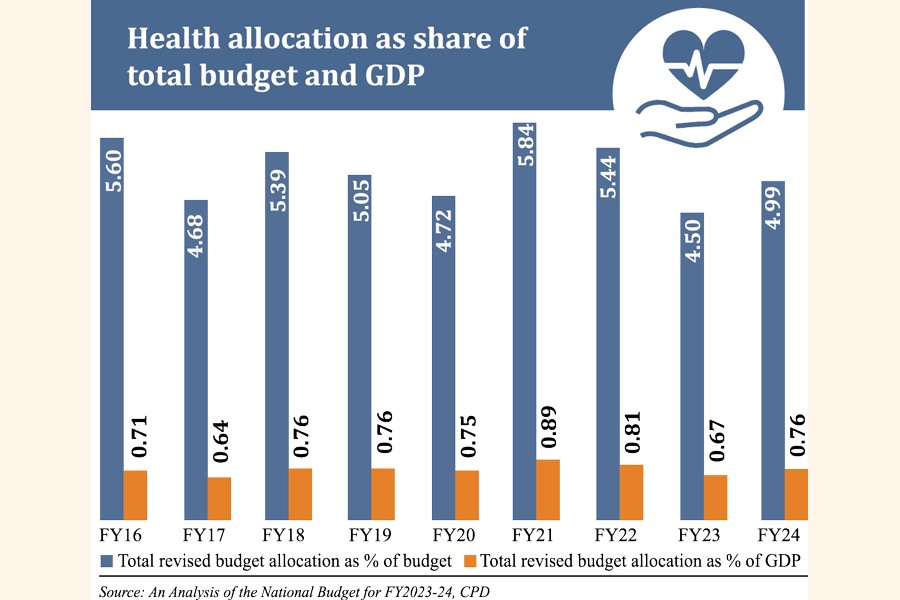
Implementation of the recommendations presented here will no doubt entail significant investment in the health sector. With the increasing GDP and resources available to the government, Bangladesh can certainly afford to invest more in quality health service delivery. The government's current budget allocation for health, at just 5.4 per cent of total public spending, is far below the WHO recommended level of 15 per cent. Even out of this limited amount of allocation typically about 20-30 per cent remains unutilized. In the immediate term, the government can deliver more by implementing the budget in full and by avoiding duplicative allocations. At the same time, the government must gradually increase budgetary allocations for the health sector, preferably by the equivalent of 1 per cent of the national budget each year, over the next several years, to reach the WHO-recommended target.
Of the total health expenditure of Bangladesh, 25 per cent goes to primary health care, 39 per cent to secondary and 36 per cent to tertiary health care. On the other hand, it is found that the largest share of the country's healthcare seekers are in want of primary healthcare. The structure of resource allocation must be rethought in view of this, and allocation for primary health care needs to be increased to 35-40 per cent of the total by the end of the Eighth FYP. Bangladesh will eventually need to transition from its current supply-side financing model towards demand-side financing. Bolder and more extensive plans are needed for this based on the current experience of SSK.
Regrettably, over the last decade or so there has been a gradual distancing between government and the civil society in the health sector. A stronger role by the civil society which is fragmented and without bold leadership at the moment, along with more openness on the part of policymakers to listen to the voice of the civil society and their recommendations, could lead to the emergence of strong win-win public-non-state actor partnerships in health service delivery. At the same time, a more open-minded bureaucratic leadership is required to break the barriers of bureaucratic control and traditional thinking, overcome vested interests and introduce new ways of doing things by involving a whole-of-society approach.
Without a healthy and productive workforce, the country can not realise its development potential and attain the targets set out in Bangladesh Vision 2041. Achieving the objectives of UHC within a reasonable time frame must be seen as a critically important milestone in Bangladesh's mid-term journey. This work needs to start without delay and in a collaborative manner involving all relevant stakeholders both within and outside of the health sector. A strong time-bound political commitment is a must if the UHC is to become a reality in Bangladesh in the foreseeable future.
This is a slightly abridged version of a policy brief which is prepared by a team with Dr Mushtaque Raza Chowdhury, Core Group Member, Citizen's Platform, and Convener, Bangladesh Health Watch, as Chair and Dr Yasmin Ahmed, Adviser, Bangladesh Health Watch, serving as the Penholder Expert. Other team members are: Mr Faruque Ahmed, Former Executive Director, BRAC International; Professor Hasnat M Alamgir, Head, Public Health, State University of Bangladesh; Dr Syed Abdul Hamid, Professor, Institute of Health Economics, University of Dhaka; Mr Rafiqul Islam, Programme Manager, Sightsavers Bangladesh; Dr Sabina F Rashid, Professor and Dean, BRAC James P Grant School of Public Health; Professor Dr Rashid-E-Mahbub, Chairman, National Committee on Health Rights Movement and Former President, Bangladesh Medical Association (BMA); Dr Lima Rahman, Director, Health, Nutrition & HIV/AIDS Sector, Save the Children in Bangladesh; Dr Sohana Shafique, Assistant Scientist, Universal Health Coverage, International Centre for Diarrhoeal Disease Research, Bangladesh (ICDDR,B); and Dr Dibalok Singha, Executive Director, Dustha Shasthya Kendra (DSK).
The initiative was led by Dr Debapriya Bhattacharya and Professor Mustafizur Rahman,
Distinguished Fellows at the CPD.
mustafiz223@gmail.com
© 2026 - All Rights with The Financial Express