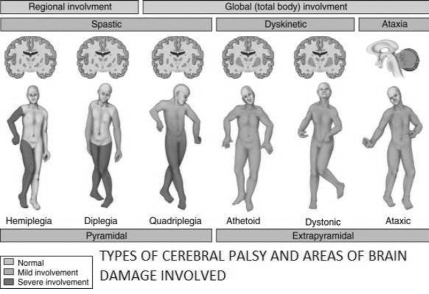
 Types of Cerebral Palsy
Types of Cerebral Palsy Nisa, a 2 years old child, came to get admitted at CRP on 10th October 2015. After coming she was diagnosed to have Dyskinetic Cerebral Palsy. Dyskinetic Cerebral Palsy results from damage to the basal ganglia of the brain. The basal ganglia is like the brain’s switchboard for interpreting messages between the movement centre and the spinal cord – it is responsible for regulating voluntary movements.
However, Nisa continued to have Occupational Therapy for being independent in his daily life from that day. Occupational Therapy focuses on optimizing body function, improving posture, and making the most of a child’s mobility. Occupational therapists help to meet everyday activities such as eating, dressing, toileting and participating in day-to-day activities.
At first Nisa’s condition was very difficult. She couldn’t eat normal food and use both of her hands. She was not able to grasp and hold and release anything. She also couldn’t sit, stand and speak. Nisa attended Occupational Therapy sessions and her condition is improving day by day. She continued therapy for 6 months. Now, she can sit independently and grasp many things by using both the hands. Nisa can eat normal food. She can also play in standing position with minimum support. Nisa’s balance is more improved than previous state and she will also improve if she continues therapy.
Not only Nisa everyday many patients with Cerebral Palsy come to Centre for the Rehabilitation of the Paralyzed (CRP) for better treatment. CRP is the only rehabilitation centre in Bangladesh where patients get best therapeutic treatment from qualified therapists who have completed bachelor degree.
What is Cerebral Palsy (CP)?
Cerebral Palsy or CP is the paralysis of brain. It is a set of neurological conditions that cause physical disability in human development - they affect the brain and nervous system. The word cerebral refers to the area in the brain that is affected, while palsy means complete or partial muscle paralysis, frequently accompanied by loss of sensation and uncontrollable body movements or tremors. Cerebral also means related to the brain or cerebrum. Cerebrum is a Latin word meaning “brain; top of the head, skull”. In the medical science the cerebrum is the anterior (front) portion of the brain consisting of two hemispheres; it is the dominant part of the brain in humans.
Children with CP exhibit a wide variety of symptoms, including:
l Lack of muscle coordination when performing voluntary movements (ataxia);
l Stiff or tight muscles and exaggerated reflexes (spasticity);
l Weakness in one or more arm or leg;
l Walking on the toes, a crouched gait, or a “scissored” gait
l Variations in muscle tone, either too stiff or too floppy;
l Excessive drooling or difficulties swallowing or speaking;
l Shaking (tremor) or random involuntary movements;
l Delays in reaching motor skill milestones; and
l Difficulty with precise movements such as writing or buttoning a shirt.
What are the causes of Cerebral Palsy?
There are some medical conditions or events that can happen during pregnancy and delivery that may increase a baby’s risk of being born with Cerebral Palsy. These risks include:
l Low birth weight and premature birth
Premature babies (born less than 37 weeks into pregnancy) and babies weighing less than 5 ½ pounds at birth have a much higher risk of developing Cerebral Palsy than full-term, heavier weight babies. Tiny babies born at very early gestational ages are especially at risk.
l Multiple births
Twins, triplets, and other multiple births — even those born at term — are linked to an increased risk of Cerebral Palsy. The death of a baby’s twin or triplet further increases the risk.
l Infections during pregnancy
Infections such as toxoplasmosis, rubella (German measles), cytomegalovirus, and herpes, can infect the womb and placenta. Inflammation triggered by infection may then go on to damage the developing nervous system in an unborn baby. Maternal fever during pregnancy or delivery can also set off this kind of inflammatory response.
l Blood type incompatibility between mother and child
Rh incompatibility is a condition that develops when a mother’s Rh blood type (either positive or negative) is different from the blood type of her baby. The mother’s system doesn’t tolerate the baby’s different blood types and her body will begin to make antibodies that will attack and kill her baby’s blood cells, which can cause brain damage.
l Exposure to toxic substances
Mothers who have been exposed to toxic substances during pregnancy, such as methyl mercury, are at a heightened risk of having a baby with Cerebral Palsy.
l Mothers with thyroid abnormalities, intellectual disability, excess protein in the urine, or seizures
Mothers with any of these conditions are slightly more likely to have a child with CP.
l Breech presentation
Babies with Cerebral Palsy are more likely to be in a breech position (feet first) instead of head first at the beginning of labour. Babies who are unusually floppy as fetuses are more likely to be born in the breech position.
l Complicated labour and delivery
A baby who has vascular or respiratory problems during labour and delivery may already have suffered brain damage or abnormalities.
l Jaundice
More than 50 per cent of newborns develop jaundice (a yellowing of the skin or whites of the eyes) after birth when bilirubin, a substance normally found in bile, builds up faster than their livers can break it down and pass it from the body. Severe, untreated jaundice can kill brain cells and can cause deafness and CP.
l Seizures
An infant who has seizures faces a higher risk of being diagnosed later in childhood with CP.
Can Cerebral Palsy be prevented?
Cerebral Palsy related to genetic abnormalities cannot be prevented, but a few of the risk factors for congenital Cerebral Palsy can be managed or avoided. For example, rubella, or German measles, is preventable if women are vaccinated against the disease before becoming pregnant. Rh incompatibilities can also be managed early in pregnancy. Acquired Cerebral Palsy, often due to head injury, is often preventable using common safety tactics, such as using car seats for infants and toddlers.
Occupational Therapy intervention
l To facilitate normal development where development has been stopped
l Improve performance components e.g. muscle power, range of movement, balance, co-ordination, bilateral integration, concentration, attention, visual perception
l Enhance performance of functional activities e.g. playing, writing, feeding, dressing, washing, walking
Feeding practice
l Modify the performance context e.g. adapt the environment-special seating, wheelchair assessment, feeding and writing aids, ramp, modify play equipment.
The writer is Clinical Occupational Therapist at Centre for the Rehabilitation of the Paralyzed (CRP), Mirpur-14, Dhaka. Email: rabeya1988@gmail.com
© 2026 - All Rights with The Financial Express