JASIM UDDIN HAROON and JUBAIR HASAN | September 16, 2020 00:00:00
The coronavirus pandemic, which arrived in the country in early March, has brought to the fore a high-level regional disparity in areas of health sector management.
The disparity, unfortunately, has led to premature deaths of many and infections of tens of thousands during the ongoing pandemic.
The issue of disparity in the matters of allocation of resources needed to fight diseases, came to the fore after many Covid-19 patients lost lives for non-availability of oxygen, ICUs, sample testing facilities and proper treatment in different parts of the country.
Though Dhaka is considered an epicentre of the pandemic in Bangladesh, accounting for almost one-third of all infections, it has the lowest rate of mortality. This highlights the inequality in the health sector as far as the availability of medical facilities in different parts of the country is concerned.
The human cost of coronavirus, however, continues to mount in the country, with around 339,332 confirmed cases and 4,759 deaths until September 14, 2020.
Experts said this inequality in areas of health facilities emerged as one of the thorniest issues, fueling public resentment due to highly-centralised health-related institutions.
Besides state hospitals, private healthcare facilities in Dhaka and some in Chittagong got involved in the virus battle, as a vast swath of Bangladesh struggled to test and treat patients, thus widening disparity, they said.
The consequences were devastating for many families. Shabnam Khanom, a third-year botany student at the University of Chittagong, watched her father die in Cox's Bazar.
On May 12, her father aged 52 tested COVID-19 positive.
He was in isolation in Ukhiya. He was advised to get admitted to Chittagong Medical College Hospital at a time when his health condition had already started to deteriorate.
He had died before reaching Chittagong from the upazila.
"My father would not have died if he had proper treatment in Cox's Bazar," she said.
Abdul Baset, who lost his sibling at the Chittagong Medical College Hospital for lack of ICU, said many like his brother died without having ICUs.
"We went to the mayor of Chittagong City Corporation seeking his favour to provide an ICU to my brother, though the number of the facility was limited at the medical college."
His brother was finally was transferred to an ICU bed, but it was too late to save his life.
"I have a video captured on my mobile phone outside the window of the 'red zone' how my brother was gasping …," Mr Baset told the FE breaking into tears.
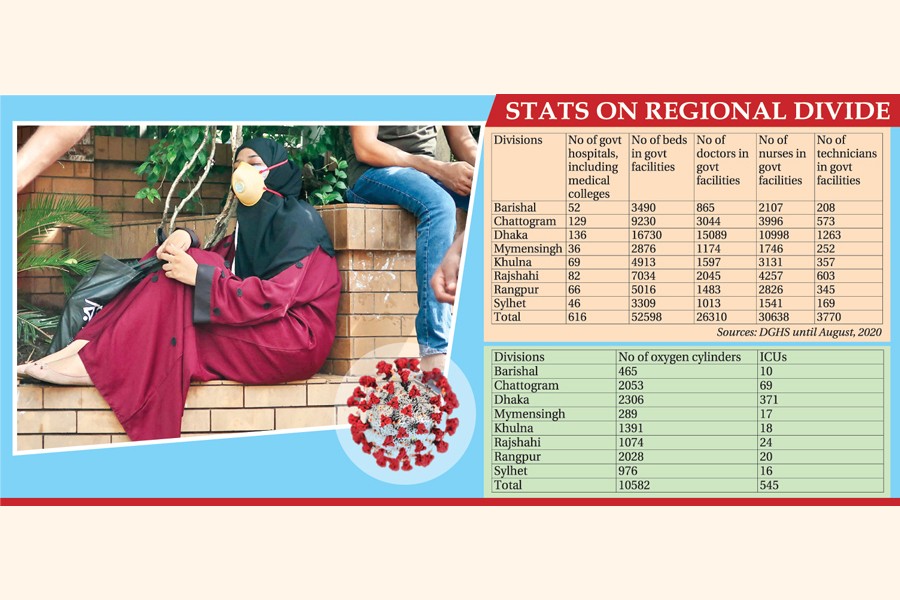
The FE has gathered official data and analysed it over the past seven weeks. It shows the healthcare disparity--division to division-district to district and even upazila to upazila-is on a stark display in terms of doctors, nurses, bed, equipment and technicians.
According to the state-run Directorate General of Health Services, the country has a total of 616 public hospitals and medical colleges.
Of the total, 43 per cent or 265 are located in Dhaka and Chittagong. The numbers are only 36, 46, 52, 66, 69 and 82 in Mymensingh, Sylhet, Barisal, Rangpur, Khulna and Rajshahi respectively.
In case of private hospitals or clinics, Dhaka and Chittagong account for half the country's 17,244 private healthcare facilities, people familiar with the issue told the FE.
In terms of doctors, there are 26,310 government physicians and 57.35 per cent and 11.56 per cent of them are posted in Dhaka and Chittagong respectively.
Half the government's nursing staff are working in these two megacities while the figure is almost the same as the number of technicians.
The disparity is more acute in case of fighting the COVID-19 pandemic as all 30 Covid-dedicated hospitals are located in Dhaka (21) and Chittagong (9).
Of testing lab facilities for detecting coronavirus infections, 63 out of 92 PCR labs are located in Dhaka, followed by 13 in Chittagong while other divisions have two or three labs each.
Admitting such disparity, senior secretary of the ministry of health and family welfare division Abdul Mannan said, "If we could deploy the existing 29,000 doctors at all the divisions in a coordinated or integrated way, probably, we would not have required to deal with such a crisis".
"We're now very serious over the matter. Nobody has been transferred to the capital from outside since I took the charge as health secretary," he said. Mr Mannan was made the health secretary in early June when the COVID-19 was almost at its peak.
Director General at the Directorate General of Health Services (DGHS) Prof. Dr Abul Bashar Mohammad Khurshid Alam echoed the secretary's assessment, saying the issue of regional disparity became more visible, especially in the wake of the pandemic.
He said it existed in the system, but it was never felt like this.
"We've been working on narrowing the gap with more fresh recruitments," the DG health told the FE.
About lesser coronavirus testing facilities outside Dhaka, DGHS additional director general Dr Nasima Sultana said they received expressions of interest mostly from Dhaka and some from Chittagong.
Dr Sultana, also president of the COVID testing committee, said Covid-19 test is being done through a real-time polymerase chain reaction (RT-PCR) machine that is quite expensive and healthcare facilities outside Dhaka might not afford it.
"Those who come to us with such required infrastructure, we allow them to do the testing, and unfortunately, they have come mostly from Dhaka and Chittagong," she added.
Such a disparity contradicts one of the basic rights guaranteed in the country's constitution. Such inequality has emerged as a serious threat to the lives of millions living in rural and semi-urban areas.
Dr SA Hamid, a professor at the Health Economics Institute of Dhaka University, said millions of people are now vulnerable to the lack of equal health care opportunities.
"A person living in Kurigram has the same right as someone who is living in Dhaka or other big cities," he said.
But Dr Hamid said all resources are centralised in Dhaka and not a single post for doctors and nurses in Dhaka is lying vacant.
"Rather, I know many doctors are staying in Dhaka in the disguise of 'attachments'."
Dr Hamid, who has spent years studying the issue, said Dhaka has been a lucrative destination for making money through private practice. Thousands of patients from different parts of the country usually come to Dhaka for treatment each day.
BSMMU associate professor (respiratory medicine) Dr Shamim Ahmed said the majority of the patients they deal with were from outside Dhaka before the pandemic as the number of modern healthcare facilities in Dhaka is far bigger than that of any other place in the country.
But the flow of patients from outside Dhaka declined significantly after the pandemic due to factors like restricted movement and fear of getting infected in the worst-hit capital city.
"Now around 15 per cent corona patients admitted here have hailed from outside Dhaka," said the associate professor at the BSMMU, a key Covid-dedicated hospital.
Professor Dr Ehteshmul Haque, an immediate past director at privately owned Anowar Khan Hospital at Dhanmondi, said they converted their hospital as a fully dedicated COVID-19 one on May 18.
"But we received dozens of patients from the Chittagong region and we had an occupancy rate of 100 per cent following day (May 19)," he said
He said even many started to lobby for getting a seat.
Although Dhaka division hosts more than one-third of the overall tally of coronavirus infections, its death rate is among the lowest due mainly to better facilities, according to health experts.
As of August 31, 2020, Barishal, an under-developed region, has the highest death rate of 2.20 per cent, followed by Chittagong (2.19 per cent), Khulna (1.91 per cent), Rangpur (1.87 per cent), Sylhet (1.80 per cent), Dhaka (1.72 per cent), Rajshahi (1.64 per cent) and Mymensingh (1.55 per cent), according to the DGHS.
Explaining the disparity, former president of Bangladesh Medical Association (BMA) Rashid-e-Mahbub said the majority of the hospitals and clinics are being concentrated mainly on Dhaka and Chittagong.
There are some healthcare bases in other regions but enough human resources are not there, he said.
Secretary-general of the BMA Dr Md Ehteshamul Huq Choudhury said healthcare professionals do not want to get posted in least-developed areas like Sunamganj, Satkhira, hilly districts and Kurigram.
"How can we solve this problem?" he raised the question before giving some possible options.
To make his case, Dr Chowdhury said the authorities of the medical colleges can encourage medical students of the least-developed regions by giving them additional marks in the exams.
The condition will be like they have to serve in primary, secondary and tertiary level health facilities in these regions and cannot apply for going to other districts, he said.
According to his second option, the government set up medical colleges in each district and it can make it mandatory for students that those who will study there will be serving in that district.
"We can look for these options for a certain time until it is saturated. The decision on this matter must come from the high-ups of the government and it must be approved by parliament," he said.
The BMA secretary-general also came up with the third option that many posts of doctors and nurses are still vacant in almost all districts in the least-developed areas.
He said the government can easily reduce the gap with appointing unemployed doctors and nurses under the government pay scale.
"We have 40,000 unemployed doctors and we must recruit them in the needy areas and the condition will be the same. So, we've problems and options too," he added.
DGHS director (admin) Dr. Sheikh Hasan Imam said the disparity in getting medicare services has long been hurting the sector, but it became more pronounced through the Covid-19.
Giving his personal opinion over the situation, he said they need to equip the district sadar hospitals so that people, except in critical cases, in the periphery do not go to divisional headquarters or Dhaka.
"The burgeoning load on divisional headquarters, namely Dhaka and Chittagong, needs to be reduced as quickly as possible. It is nothing impossible because we have the infrastructure. What we require to do is to remove the human resource deficiency," he said.
A study based on the Health and Demographic Survey in 2014 said Bangladesh has over 70 per cent disparity in health care measured by Gini coefficient.
jasimharoon@yahoo.com
jubairfe1980@gmail.com
© 2026 - All Rights with The Financial Express