 A doctor is examining a dengue-effected child at a hospital in Dhaka —bdnews24.com Photo
A doctor is examining a dengue-effected child at a hospital in Dhaka —bdnews24.com Photo A new OECD report gives us a useful opportunity to look more closely at the extent of skilled-worker migration from Bangladesh to advanced economies. The report, International Migration Outlook 2025, compiles comparable data on international migration across Organization of Economic Cooperation and Development (OECD) countries. It also covers the movement of doctors and nurses, which is especially relevant for Bangladesh. The purpose of this article is to use the report to place Bangladesh’s experience in context, both in relation to its South Asian neighbours and to broader global trends.
According to the OECD, around 4,900 Bangladeshi doctors or physicians were working in OECD countries in 2020-21. This is more than double the number recorded in 2000, when just over 2,100 Bangladeshi doctors were employed abroad. A similar pattern appears among nurses. Roughly 3,100 Bangladeshi nurses were working in OECD countries in 2020-21, compared to fewer than 700 two decades earlier. Overall, these figures point to a steady and persistent outward movement of trained health professionals over time.
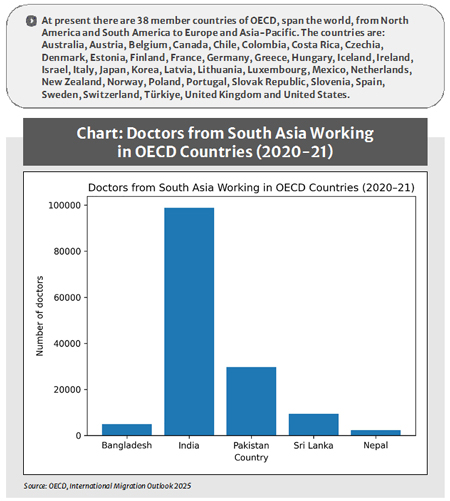
The discussion becomes clearer when Bangladesh is viewed alongside other South Asian countries (see the chart) .Seen alongside other South Asian countries, Bangladesh’s numbers appear relatively modest. India had close to 99,000 doctors working in OECD countries in 2020-21, while Pakistan had around 30,000 and Sri Lanka roughly 9,500. Bangladesh’s figure is far smaller in absolute terms. This difference in scale may help explain why the issue receives relatively limited attention in public debate, as Bangladesh does not stand out as a major exporter of doctors when compared with India.
However, absolute numbers tell only part of the story. The OECD also estimates expatriation rates, which measure the share of a country’s doctors working abroad relative to its total stock. For Bangladesh, this rate is estimated at around four to five per cent. India’s corresponding figure is close to nine per cent, Pakistan’s just over ten per cent, and Sri Lanka’s considerably higher at about 26 per cent. Nepal, while smaller in absolute numbers, also shows a relatively high share of its doctors working abroad.
At first glance, Bangladesh’s position may seem reassuring. Its expatriation rate is lower than that of several neighbours. But this comparison needs to be handled with care. Bangladesh begins from a much lower doctor-to-population ratio, at roughly 0.8 doctors per 1,000 people, compared with around 0.9 in India and about 1.2 in Sri Lanka. Losing a smaller share from a thinner base can still place significant strain on the health system, particularly outside major urban centers where health facilities often struggle with inadequate staff and limited specialist coverage.
More importantly, migration does not affect all doctors equally. Those who leave are rarely new graduates. They are often doctors who have completed postgraduate training, gained several years of experience, and reached a stage where their skills are both mature and internationally recognised. These are typically doctors in their thirties and forties, who play an important role in district hospitals, supervise junior colleagues, and manage complex cases, often with limited resources.
When such doctors leave, the impact is not easily captured by national averages. A relatively small number of departures can weaken entire departments, particularly in smaller hospitals. The loss, therefore, is larger than the raw percentages suggest, even if the overall scale appears manageable.
 The OECD report also helps place Bangladesh’s experience in a broader global context. In OECD countries, foreign-born doctors now account for roughly one quarter of the medical workforce, and nearly one in five doctors is foreign-trained. This share has increased steadily over the past two decades. Ageing populations, rising demand for healthcare, and large numbers of retiring doctors mean that many advanced economies now depend structurally on international recruitment to sustain their health systems.
The OECD report also helps place Bangladesh’s experience in a broader global context. In OECD countries, foreign-born doctors now account for roughly one quarter of the medical workforce, and nearly one in five doctors is foreign-trained. This share has increased steadily over the past two decades. Ageing populations, rising demand for healthcare, and large numbers of retiring doctors mean that many advanced economies now depend structurally on international recruitment to sustain their health systems.
Seen in this light, Bangladeshi doctors appear to be responding to opportunities created by global demand rather than simply reacting to conditions at home. Doctors are leaving not because Bangladesh is uniquely dysfunctional, but because demand for medical professionals has been growing steadily across much of the developed world.
Comparisons within South Asia help clarify this point. India exports doctors on a large scale, but it also manages to retain many by offering a wide range of professional opportunities, particularly in the private sector. Migration there is often temporary or takes a more circular form. Sri Lanka, by contrast, has a strong public medical education system but more limited career progression at home, which appears to contribute to its high expatriation rate. Pakistan shares some similarities with Bangladesh, especially its close links to the UK health system and the gradual outflow of mid-career doctors.
Bangladesh lies somewhere between these cases. It does not experience dramatic exits, but it does experience gradual and persistent losses. Because the movement is steady rather than sudden, it rarely forces a clear policy response. Hospitals adapt as best they can. Remaining doctors often take on more responsibilities. Patients may travel further or wait longer for care. Over time, these adjustments become part of the routine, and the underlying loss of capacity becomes harder to see.
This gradual pattern is part of what makes the issue difficult to address. At the same time, the OECD data suggest that global demand for doctors is likely to grow rather than ease in the coming years. As populations continue to age in Europe and North America, competition for medical professionals is expected to intensify. In that context, Bangladesh’s relatively modest expatriation rates today may not remain modest indefinitely.
Preventing doctors from leaving altogether is neither realistic nor desirable. International mobility has become a normal part of professional life in medicine. A more practical focus, therefore, is on retaining doctors for longer, particularly during the mid-career years when their contribution to the health system tends to be greatest.
That shift moves attention away from dramatic interventions and towards more ordinary questions: how promotions work, how postings are decided, whether hospitals function as intended, and whether professional effort is recognised in consistent ways. Doctors do not leave only because salaries are higher abroad. Often, it is the predictability of systems, clearer training pathways, and a sense of steady career progression that matter just as much.
The OECD figures do not suggest that Bangladesh is failing in isolation. They point instead to a quieter challenge. Bangladesh has become part of a global market for medical labour without fully adapting to it. As long as the losses remain manageable, the system tends to absorb them. But absorption should not be confused with sustainability.
Bangladesh is producing doctors the world wants. The open question is whether it can also create the conditions needed for enough of them to remain, long enough, to support the health system at home.
The writer is an economist and independent researcher.
syed.basher@gmail.com
© 2026 - All Rights with The Financial Express